At-A-Glance
- 50 years ago, anti-reflux surgery was recommended for anyone with hiatal hernia, but that is no longer the case.
- Hiatal hernia is extremely common in people who have reflux as well as those who do not.
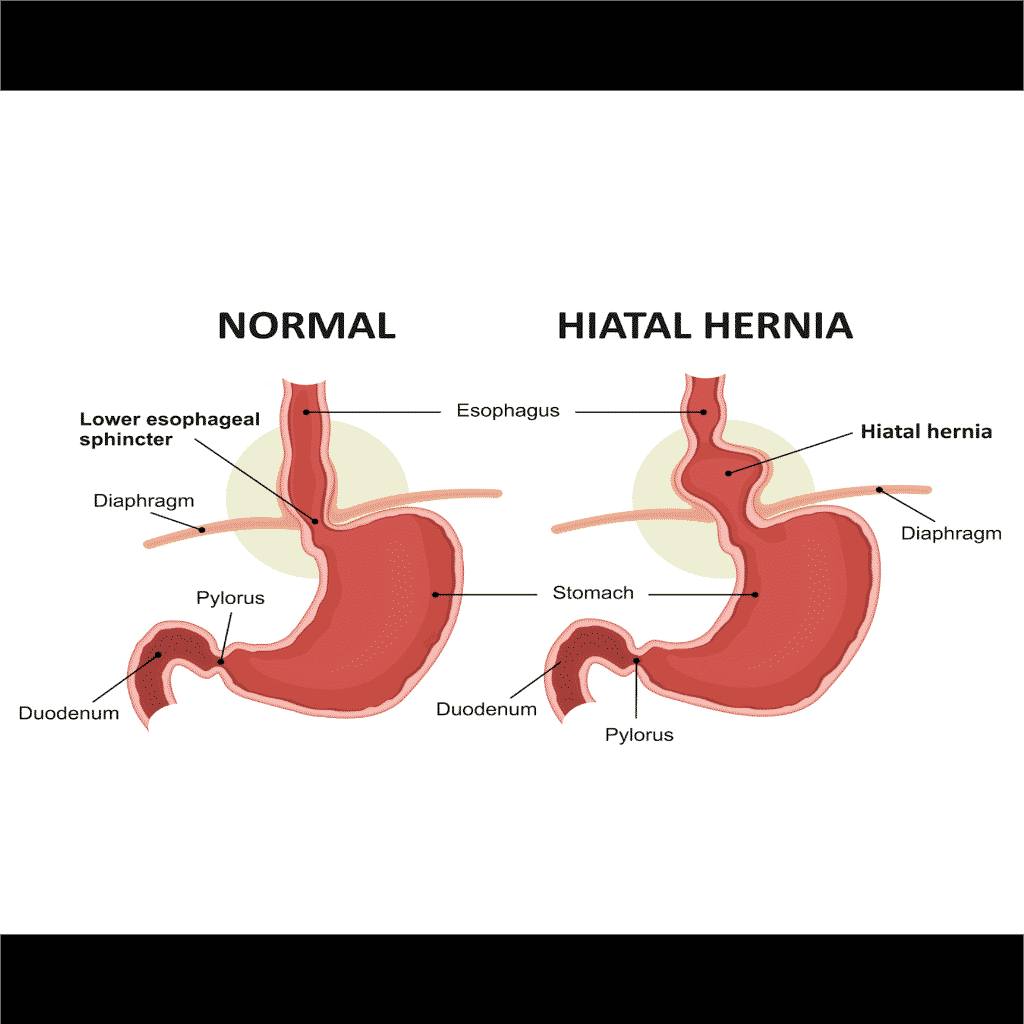
- Under normal circumstances, the stomach valve (lower esophageal sphincter, LES) is precisely at the diaphragm, and the diaphragm (as a sling) contributes about one third of the strength of the LES (see above). Under normal circumstances, this valve prevents the reflux (back-flow) of stomach contents into the esophagus (swallowing tube) and throat.
- Although this is often poorly understood, having anti-reflux surgery should no longer depend on the presence or absence of a hiatal hernia, aka hiatus hernia.
Hiatal hernia, also called hiatus hernia, is a confusing topic in medicine, particularly regarding acid reflux and the significant factors that contribute to it.
Around 50 years ago, anti-reflux surgery was recommended for anyone with hiatal hernia, but that is no longer the case.
While it is true that the diaphragm provides some of the “pinch-cock” effect/strength of the lower esophageal sphincter (LES), it is no longer considered to be a major cause of acid reflux.
People can have a hiatal hernia without reflux. Furthermore, how it is demonstrated by x-ray depends upon how the x-rays are obtained. In other words, x-rays can be misleading based how the valve itself is stressed during the x-ray. Pushing on the stomach during the x-ray study, for example, is more likely to show a hiatal hernia quite often with no clinical significance. << That’s a very important sentence!
To some extent, the significance depends upon the size of hernia. Hernia occurs when the lower esophageal sphincter – the stomach valve – is above the diaphragm. For most people with a hiatal hernia smaller than 4 centimeters, it is not a significant reflux-causing variable, and it does not require surgical treatment.
In summary, hiatal hernia is not a true hernia that requires surgical repair. It is extremely common in his identification often depends upon how swallowing x-rays are performed. It is a factor for reflux, but certainly not the critical fact. To control reflux, just follow the well-researched effective diet and lifestyle modifications.
Why Does A Reflux Diagnosis Take So Long?
Part of this issue is due to medical specialization.
The trend towards medical specialization has intensified over the last 50 years… while simultaneously disenfranchising primary care physicians (PCPs). Each specialist – including lung doctors, ENT doctors and GI specialists – just takes care of one part of the body. This has led to specialists who are unable to diagnose / treat reflux because they don’t understand how the respiratory and digestive tracts are connected. They are directly connected at the upper esophageal valve, which is supposed to protect against reflux in the throat. There is also a direct connection between the throat and the lungs at the level of the vocal cords.
I have taken care of thousands of patients with reflux over the course of my career, and almost all have seen multiple specialists including PCPs, allergists, otolaryngologists, pulmonologists, and gastroenterologists.
What to Do About Reflux
WARNINGS:
– Don’t take PPIs!
– Understand that acid reflux increases your risk of esophageal cancer, so get screened
Reflux is curable with effort and commitment to change.
I’ve written four books about these topics: Dropping Acid: The Reflux Diet Cookbook & Cure, The Chronic Cough Enigma, Dr. Koufman’s Acid Reflux Diet, and Acid Reflux in Children.
However, here are the most important pieces of advice I can offer:
- No eating or drinking within five hours of going to bed
- Sleep on an incline no less than 45-degrees (gravity helps)
- Eat five small meals
- No fried or high-fat foods
- No alcohol, chocolate or soft drinks (including fruit juice) of any kind
- Take Pepcid 20 mg. before each meal and before bed
- Take a tablespoon of Gaviscon Advance Aniseed after each meal and before bed (not available in stores in the U.S., but available online)
- Drink alkaline water as much as you conveniently can: an alkaline pitcher is convenient (and test it with pH paper or a pH tester to make sure it’s 8.0 or greater)
- Chew sugar-free gum after eating or drinking anything but water.
If you’ve read at least one of my books and you’re following this guidance and you still need help, you can book a consultation with me.








